

BACKGROUND:
Multiparameter flow cytometry (MFC) has increasingly been used for measurable residual disease (MRD) assessment in patients with acute myeloid leukemia (AML), while next-generation sequencing (NGS)-based MRD monitoring tool is in clinical development for its application. Clonal hematopoiesis (CH), in which leukemia-associated somatic mutations gene are present in individuals with no apparent hematologic disease, adds a challenge in the detection of MRD. In patients with AML, CH could be potentially pre-leukemic, while persistent mutations in DNMT3A, TET2 orASXL1 (DTA) in remission marrow are usually removed from the analysis of residual leukemic cells. However, reports suggest that persistent DTA mutations in remission may be correlated with an increased relapse risk.
In the patients with DTA mutations, the use of NGS for MRD monitoring is limited or modified due to the presence of CH clone in the remission marrow. We evaluated whether MFC-MRD can be adjunctive to predict the risk of AML relapse in this population of 221 patients with DTA mutation (DNMT3A (n=123), ASXL1 (n=56) or TET2 (n=100).
METHODS:
The present study evaluated long-term outcomes in AML patients who achieved first complete remission (CR1) and compared outcomes according to MFC-based MRD status (was defined as negative if patients achieved 0.1 or less) assessed at the time of CR1.
A total of 435 patients diagnosed with AML and treated with induction chemotherapy between 2015 and 2018 were included. MFC-MRD was assessed in 336 patients in CR1 (77%). NGS was performed using samples obtained at the time of initial diagnosis and used for mutational subgroup classification.
Overall survival (OS) was calculated as the date of CR1 to the date of death and censored on the date of the last follow-up. Relapse-free survival (RFS) was defined as the time from the date of CR1 to the date of relapse or death from any cause. Cumulative incidence of relapse (CIR) and non-relapse mortality (NRM) were calculated considering competing risk. The Kaplan-Meier method using a log-rank test and a multivariate Cox proportional hazard model was used for analyses of time-to-event endpoints. For CIR and NRM, Gray test was performed for the risk factors and the Fine-Gray model was adopted for the multivariate model.
RESULTS:
According to the MFC-MRD status, i.e., the group with positive MRD (MRDpos; n=118, 35%) vs. those with negative MRD (MRDneg; n=218, 65%), we evaluated OS, RFS, and CIR. The MFC-MRDneg group showed better OS at 2 years 67.0% than the MFC-MRDpos group 40.7% (p<0.001). The MFC-MRDneg group also showed a higher RFS rate at 2 years (58.7%) than the MFC-MRDpos group (40.6%) (p=0.001). The CIR was higher in the MFC-MRDpos group, 26.9%, than in the MFC-MRDneg group 21.1%, but with borderline statistical significance (p=0.083). NRM was slightly higher in the MFC-MRDpos group, 32.5%, than in the MFC-MRDneg group, 20.2%, but with borderline statistical significance (p=0.057).
We divided the groups according to the number of induction treatment courses, AML type, cytogenetics risk, and age (<60 vs ≥60), and compared OS, RFS, CIR and NRM between MFC-MRDpos vs MRDneg groups, which showed that MFC-MRD is relevant for risk stratification regardless of above-mentioned clinical variables Tab1.
Also, we evaluated MFC-MRD status at CR by mutational profile subgroup. Long-term outcomes such as OS, RFS, CIR or NRM were compared by the mutational subgroup. It consistently showed a trend of superior OS, RFS and lower risk of CIR in patients with MFC-MRDneg compared to MFC-MRDposTab1.
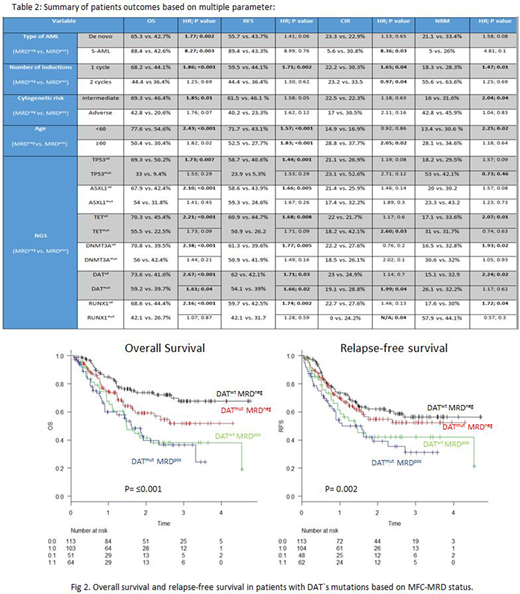
Of interest, in the subgroup of patients carrying any DTA mutations (n=221), those with MFC-MRDneg (n=103) showed better OS (HR 1.61 [1.01-2.55%]; p=0.042), RFS (HR 1.66 [1.06-2.61%]; p=0.026) and CIR (HR 1.99[1.03-3.83%]; p=0.04) compared to those MFC-MRDpos (n=64; Fig 1). Multivariate analysis confirmed that the MFC-MRDneg is an independent prognostic factor in patients with DTAmutwith respect to OS: MFC-MRDpos (HR 1.63, p=0.04) and age (≥60; HR 2.04, p=0.008) for OS; for RFS, MFC-MRDpos (HR 1.71, p=0.02) and age (≥60; HR 2.32, p= 0.001); for CIR, MFC-MRDpos (HR 2.31, p=0.01) and HCT (HR 0.14, p=<0.001).
Conclusion: These findings suggest that in AML patients with DTAmut, MFC-MRD status at the time of remission assessment can be a tool for MRD assessment when NGS-based MRD assessment is limited. Further study is strongly warranted to reach a clearer conclusion with multiple cohorts.
Schimmer:Takeda: Honoraria, Research Funding; Novartis: Honoraria; Jazz: Honoraria; Otsuka: Honoraria; Medivir AB: Research Funding; AbbVie Pharmaceuticals: Other: owns stock . Tierens:Amgen: Membership on an entity's Board of Directors or advisory committees; Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees; Astellas Pharma: Membership on an entity's Board of Directors or advisory committees. McNamara:Novartis: Honoraria. Maze:Pfizer: Consultancy; Novartis: Honoraria; Takeda: Research Funding. Gupta:Pfizer: Consultancy; Bristol MyersSquibb: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Sierra Oncology: Consultancy, Membership on an entity's Board of Directors or advisory committees; Incyte: Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal